

Background and Scientific Rationale
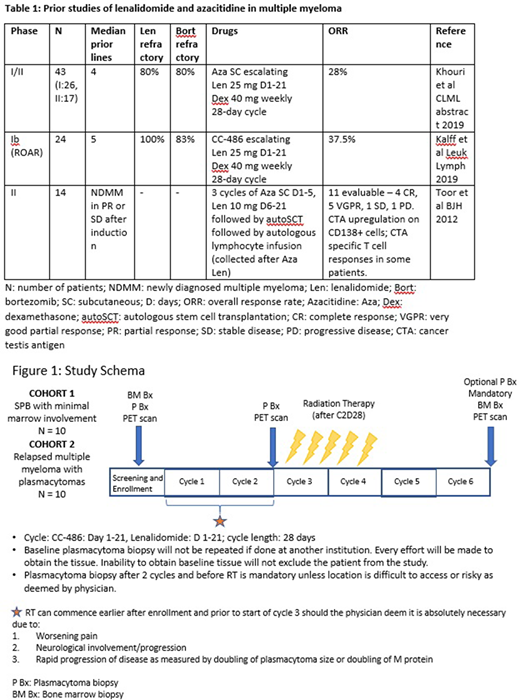
Solitary plasmacytoma of the bone (SPB) is a rare entity representing 5% of all plasma cell dyscrasias. SPB treated with radiation therapy (RT) has a 10% risk of progression to multiple myeloma (MM) over 3 years if there is no marrow involvement, whereas there is a 60% chance of progression over 3 years in patients with minimal marrow involvement. Median time to progression in the latter group is 26 months. Presently, despite mounting evidence of a significant risk of progression to MM, there is no FDA-approved therapy and patients are usually treated with localized RT. This is an area of unmet need. A similar opportunity exists in the setting of MM patients relapsing with localized disease amenable to RT. This group of patients may not immediately require long-term systemic therapy especially if RT combined with epigenetic modulation and lenalidomide results in therapeutically relevant immune responses. A few studies combining lenalidomide and azacitidine have shown responses even in a lenalidomide refractory population with upregulation of cancer testis antigen (CTA) as well as CTA specific T cell responses (Table 1).
These synergistic mechanisms focus on: 1) manipulating antigen expression and enhancing antigen presentation (both neoantigens and cancer testis antigens) with oral azacitidine (CC-486), and 2) augmentation of antigen specific immune responses via increased IL2 production leading to an increase in the proliferation of T cells with lenalidomide. This combination with RT would serve to inflame the tumor microenvironment and potentially lead to therapeutically active systemic immune responses via an abscopal effect.
Study Design and Methods
This is an open-label, single center, single-arm study of CC-486, lenalidomide plus RT, which will enroll a total of 20 patients in two cohorts.
Clinical trial registry number NCT04174196, actively recruiting.
Study population and inclusion criteria
Each cohort will enroll ten patients -
Cohort 1:
i) Histologically confirmed newly diagnosed solitary plasmacytoma of the bone or lytic bone lesion
ii) Minimal marrow involvement (Detectable clonal bone marrow (BM) plasma cells by multicolor flow cytometry and ≤ 10% clonal plasma cells in a BM biopsy by immunohistochemistry, morphology, or flow cytometry)
iii) Secretory M protein < 3 g/dL
Cohort 2:
i) Relapsed multiple myeloma with plasmacytomas appropriate for RT on imaging
ii) Relapsed (reappearance of M-spike/serum FLC) or progressive myeloma defined by a 25% increase from nadir in M-spike or involved serum FLC on 2 separate measurements; or with BM involvement by clonal plasma cells detectable by IHC
iii) Any prior number of therapies is permitted, including prior RT
iv) Allogeneic transplant patients are permitted
Statistical methods
We estimate the historical rate of stringent complete response (sCR) is approximately 5% (based on the rate for newly diagnosed myeloma with lenalidomide and dexamethasone on the MAIA study of 7.3% and for relapsed myeloma with Rd based on the POLLUX study of 4.6%).
The primary endpoint of the study will be reported separately for the two cohorts. With 10 patients in each cohort, the maximum half-width of the exact 95% confidence interval for the response rate is +/- 0.31. A sCR rate of ≥20% would be considered promising for either cohort.
Study treatment
In the study, patients will be treated with CC-486 100 mg on day 1-21 and lenalidomide 25 mg on day 1-21 for 6 cycles. RT to the plasmacytoma will be initiated after cycle 2. Total dose may vary between 30-50 Gy (45-50 Gy for cohort 1) based on clinical judgement. (Figure 1)
Endpoints
Primary
To provide preliminary efficacy data based on the rate of sCR by 2016 IMWG Criteria on post-treatment BM biopsy and aspirate specimens with no new lesions by PET.
Secondary
- To assess the safety of this combination.
- To estimate the progression free survival and overall survival
Exploratory
- To evaluate antigen expression at the tumor site pre and post RT
- To further characterize the antigen specific T cell response pre and post RT at the tumor site
- To assess changes in epigenetic marks
- To assess changes in the tumor microenvironment
Shah:Physicians Education Resource: Honoraria; Celgene/BMS: Research Funding. Mailankody:Juno Therapeutics, a Bristol-Myers Squibb Company: Research Funding; Allogene Therapeutics: Research Funding; Janssen Oncology: Research Funding; Takeda Oncology: Research Funding; PleXus Communications: Honoraria; Physician Education Resource: Honoraria. Korde:Astra Zeneca: Other: Advisory Board; Amgen: Research Funding. Hultcrantz:GSK: Research Funding; Daiichi Sankyo: Research Funding; Amgen: Research Funding; Intellisphere LLC: Consultancy. Smith:Precision Biosciences: Consultancy; Fate Therapeutics: Consultancy; Bristol Myers Squibb: Consultancy, Patents & Royalties, Research Funding. Shah:Janssen Pharmaceutica: Research Funding; Amgen: Research Funding. Lahoud:MorphoSys: Other: Advisory Board. Scordo:McKinsey & Company: Consultancy; Angiocrine Bioscience, Inc.: Consultancy, Research Funding; Omeros Corporation: Consultancy; Kite - A Gilead Company: Other: Ad-hoc advisory board. Dahi:Kite: Consultancy. Chung:Genentech: Research Funding. Hassoun:Novartis: Consultancy; Celgene: Research Funding; Takeda: Research Funding. Barker:Elekta: Research Funding; Amgen: Research Funding; Alpha Tau Medical: Other: Travel expenses, Research Funding; Merck: Research Funding. Giralt:KITE: Consultancy; MILTENYI: Consultancy, Research Funding; OMEROS: Consultancy, Honoraria; CELGENE: Consultancy, Honoraria, Research Funding; AMGEN: Consultancy, Research Funding; NOVARTIS: Consultancy, Honoraria, Research Funding; JAZZ: Consultancy, Honoraria; ACTINUUM: Consultancy, Research Funding; TAKEDA: Research Funding. Landgren:Adaptive: Consultancy, Honoraria; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; BMS: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; Glenmark: Consultancy, Honoraria, Research Funding; Juno: Consultancy, Honoraria; Seattle Genetics: Research Funding; Pfizer: Consultancy, Honoraria; Merck: Other; Karyopharma: Research Funding; Binding Site: Consultancy, Honoraria; BMS: Consultancy, Honoraria; Cellectis: Consultancy, Honoraria; Juno: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Merck: Other; Glenmark: Consultancy, Honoraria, Research Funding; Amgen: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Takeda: Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Karyopharma: Research Funding; Binding Site: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Other: Independent Data Monitoring Committees for clinical trials, Research Funding; Seattle Genetics: Research Funding; Celgene: Consultancy, Honoraria, Research Funding. Lesokhin:Janssen: Research Funding; GenMab: Consultancy, Honoraria; BMS: Consultancy, Honoraria, Research Funding; Juno: Consultancy, Honoraria; Takeda: Consultancy, Honoraria; Genentech: Research Funding; Serametrix Inc.: Patents & Royalties.
CC-486 is an is an oral hypomethylating agent that has been studied in acute myeloid leukemia. This study combines CC-486 with lenalidomide and radiation therapy in plasma cell disorders.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal